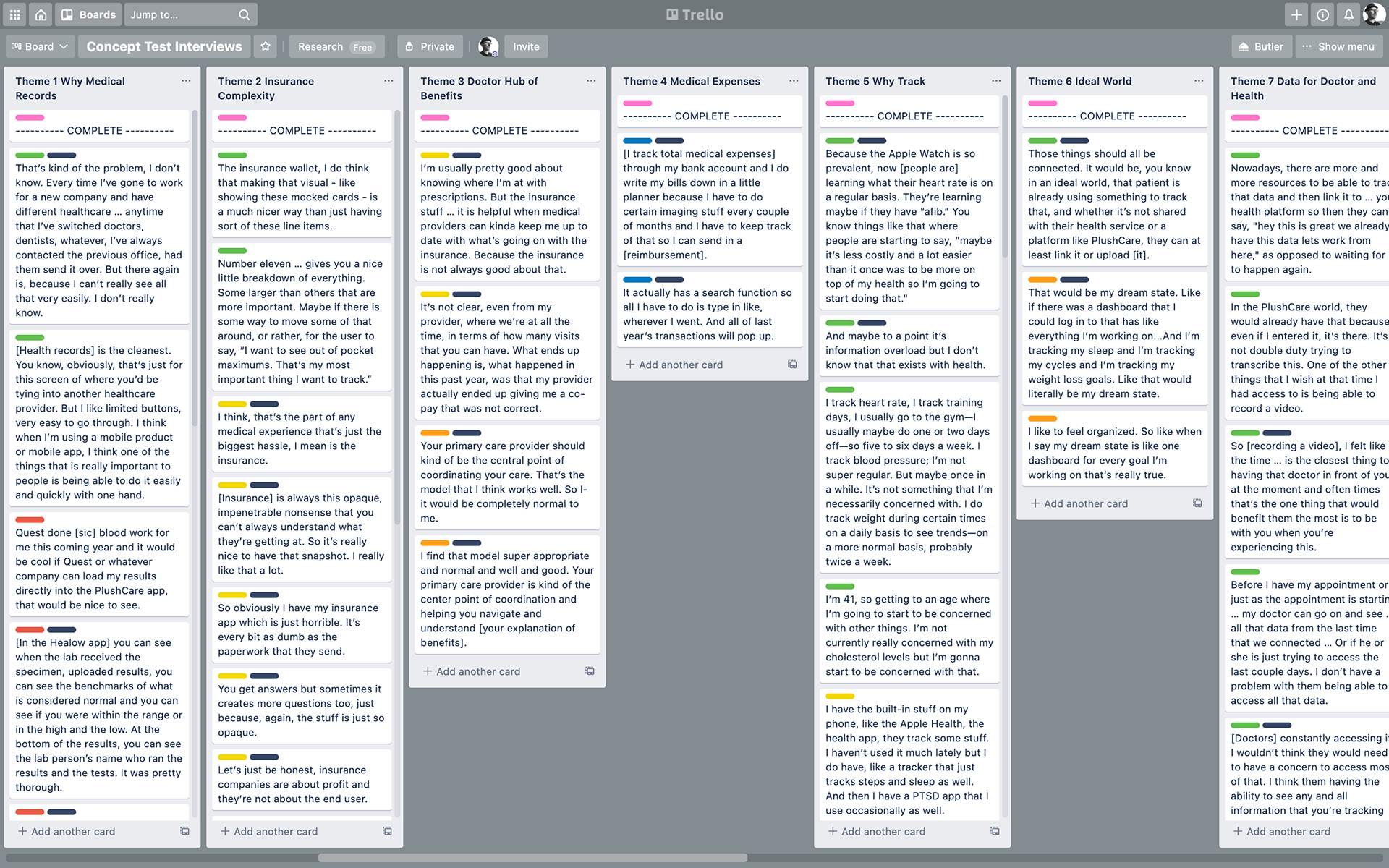
Themes identified during an analysis of qualitative data using Trello

Results of a Pew Research study indicate that about one-quarter of U.S. adults wears a smartwatch or fitness tracker.

Consumer devices that do and do not measure blood pressure.
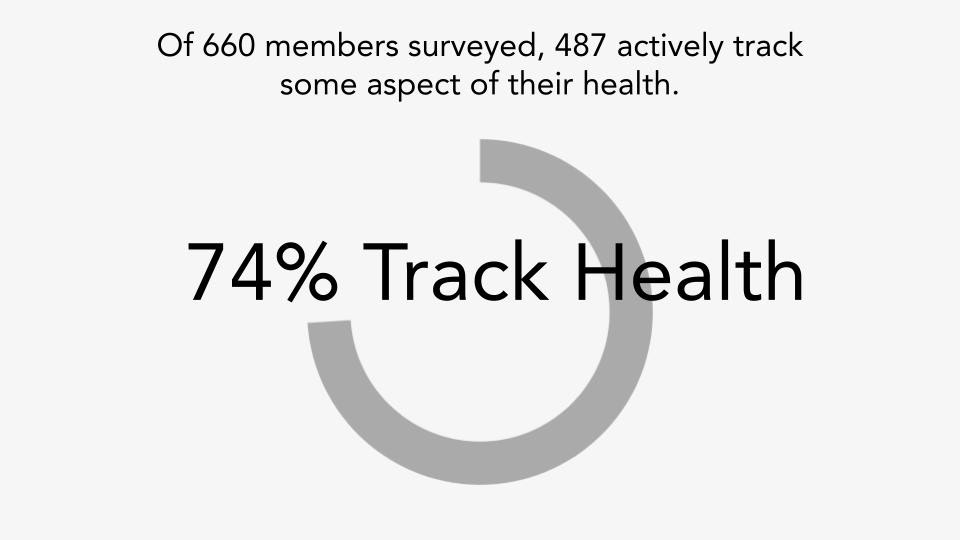
Nearly three-quarters of members surveyed tracked some aspect of their health.
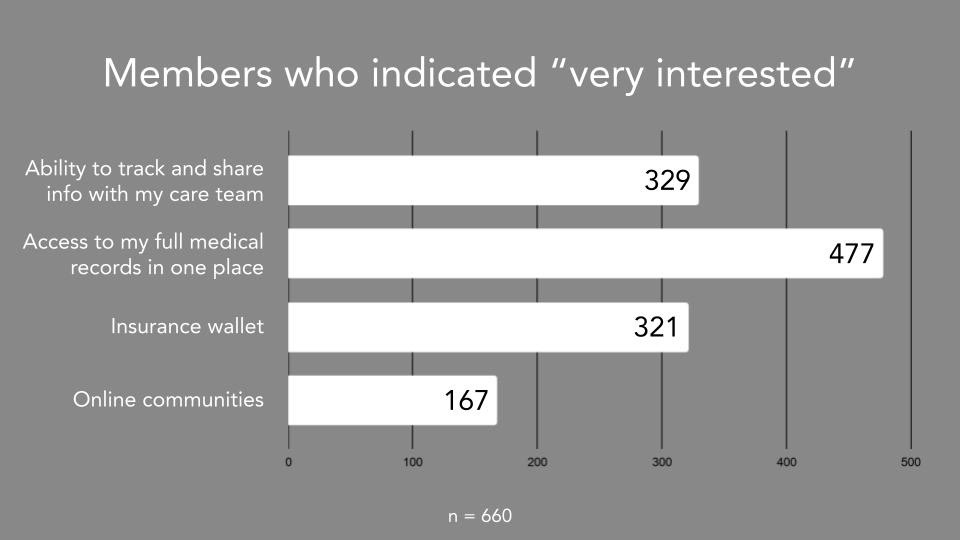
Members indicated they were "very interested" in access to medical records nearly three times that of online communities.
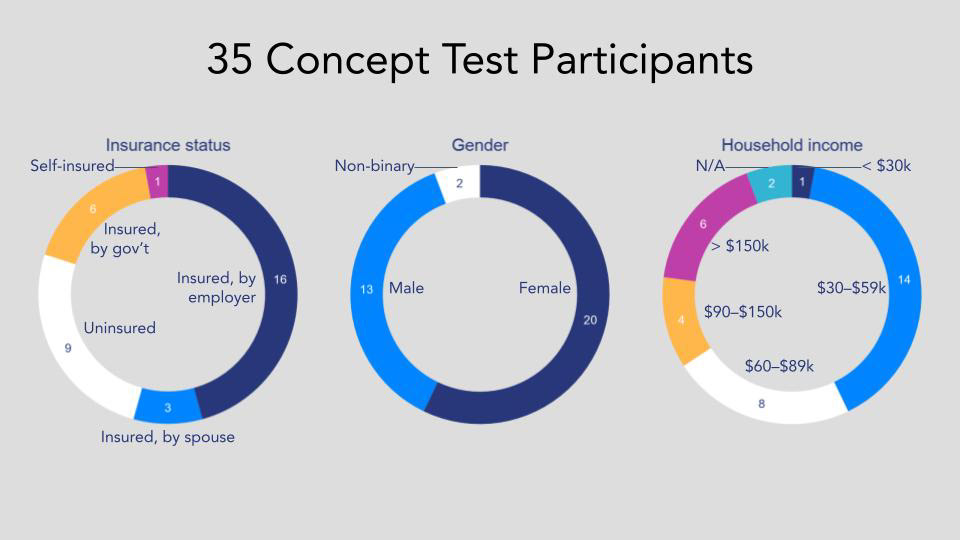
Demographic attributes of participants by insurance status, gender, and household income.
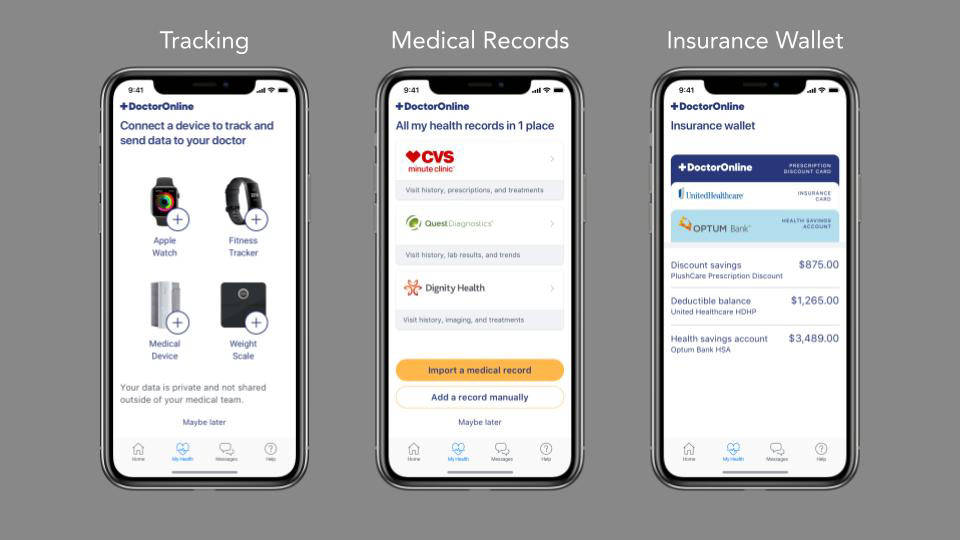
Three thematic concepts: medical records, tracking, and insurance wallet.
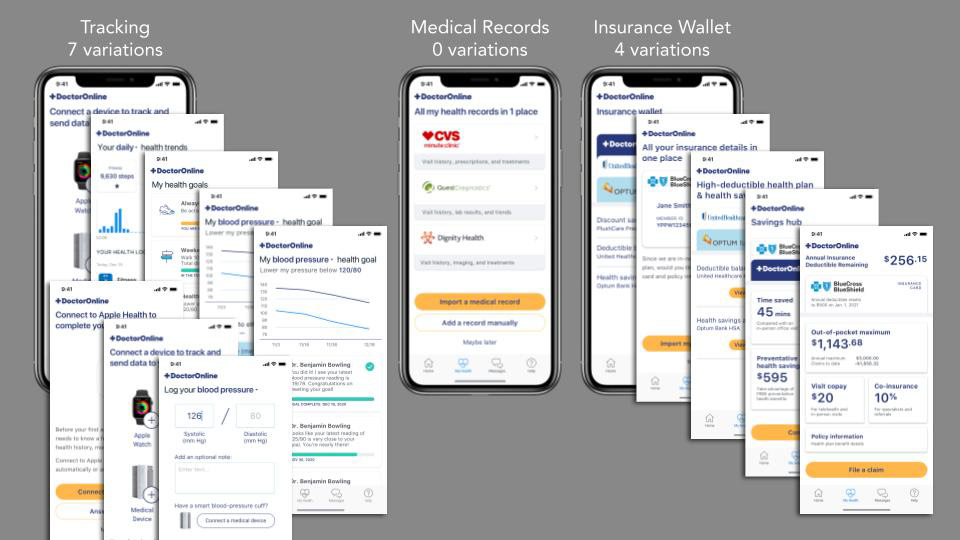
The variations provided within each theme.
An interview in progress using Google Meet.
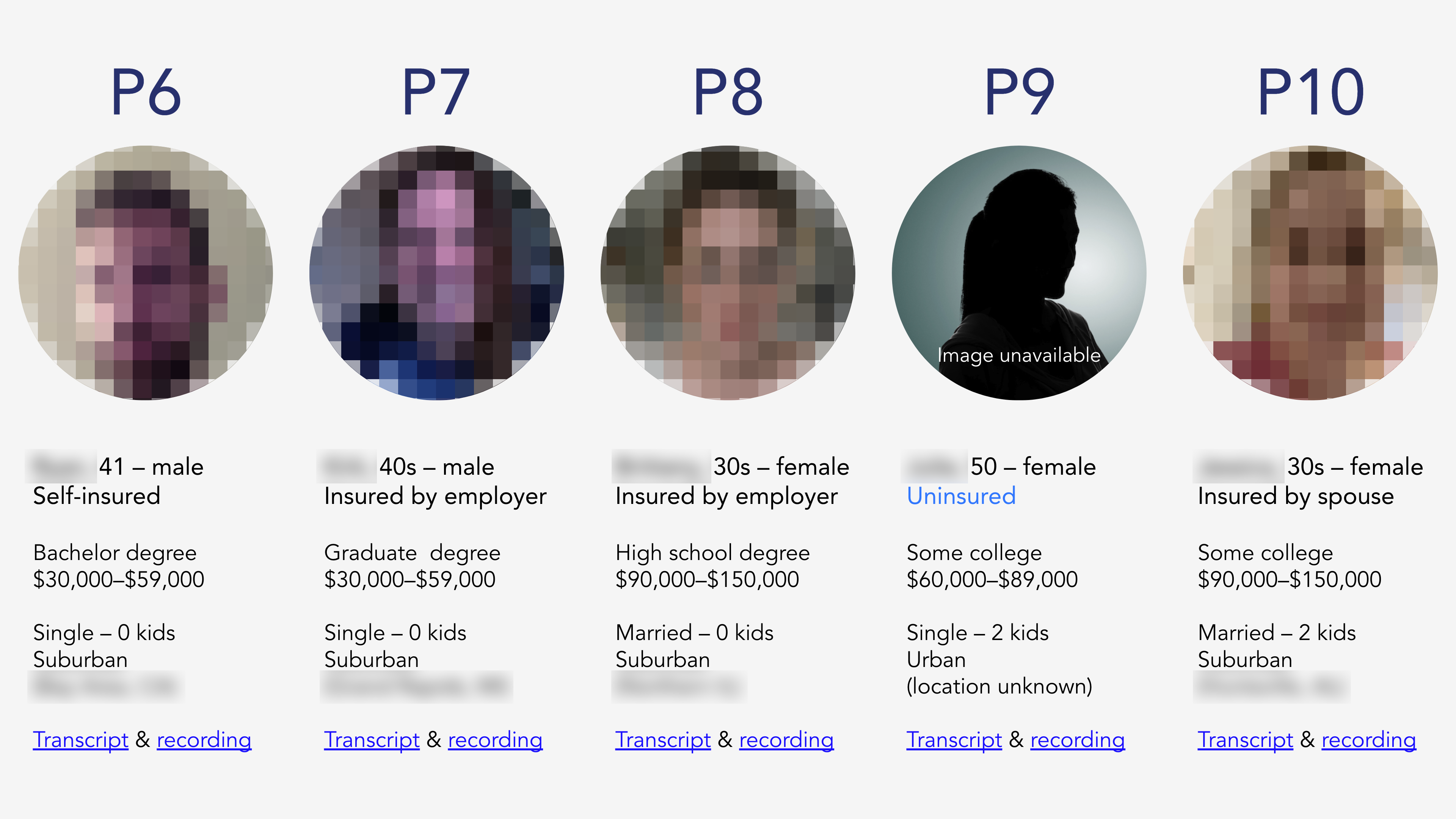
The five participants who agreed to an interview.

Trello board with raw quotes arranged by participant, ready for thematic grouping and analysis.
![Quote from P6: "[This] is showing me that, ‘Hey, Dr. Benjamin is connected to this. He’s seen this.’ There’s some confirmation that I’m entering this and it’s actually being accessed. So that feels good. I think more people would be better patients if they had more tools and resources to interact and engage with their healthcare provider. You can go on the PlushCare website, enter in notes how you feel, and you can record a quick video describe how you’re feeling. [That would be] the closest thing to having that doctor in front of you, at the moment, and often times that’s the one thing that would benefit them the most, is to be with you when you’re experiencing this."](https://cdn.myportfolio.com/b20b4dce-691a-448c-a235-fbffcf38e22b/c1042d28-1410-4f6c-a7fe-e33388ca2e6f_rw_1200.jpg?h=c6cf828e693950e57e482d2496811d76)
A direct quote from a participant about receiving feedback from a doctor outside an appointment.
![Quote from P9: "[After my husband died] I had to set up everything in my phone and it became one place for everything. With that being said, if the PlushCare app had all my records in one place, it would feel complete." Quote from P10: "I had to go and get a giant thick file of all my old files and you know [laughs], which was really just a pain. You know, brought them myself to my new doctor and you know, they were weird about it because they wanted it to be done digitally."](https://cdn.myportfolio.com/b20b4dce-691a-448c-a235-fbffcf38e22b/a0d4d080-10df-478c-beed-2a4a299893bb_rw_1200.jpg?h=d8be828bc49ba4383c1dabf52fba97d4)
Direct quotes from participants about having medical records all in one place.

Words participants used to describe their insurance.
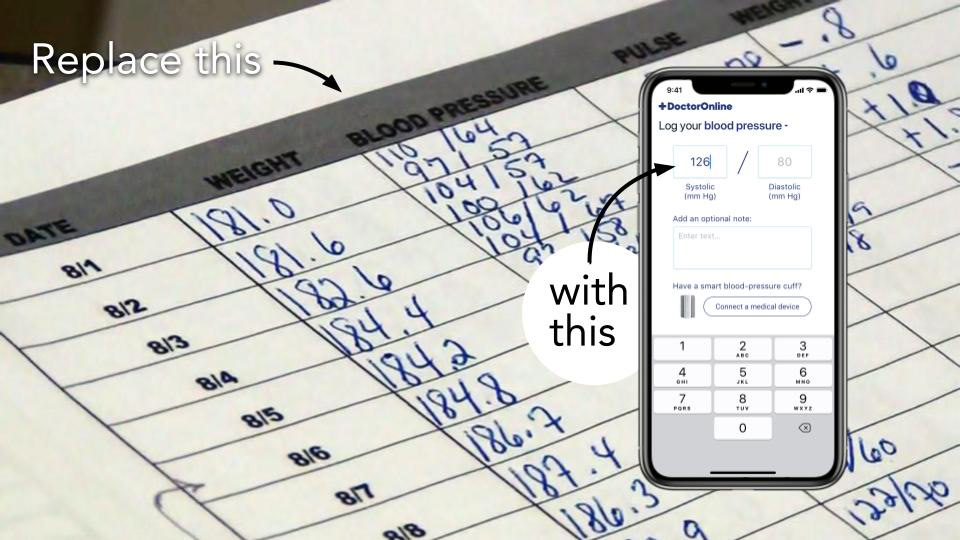
A digital product to record and track blood pressure could replace pen and paper logs.